Premature ventricular contraction
| Premature ventricular contraction | |
|---|---|
 | |
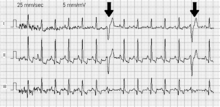
| A premature ventricular contraction marked by the arrow. | |
| Classification and external resources | |
| Specialty | Cardiology |
| ICD-10 | I49.3 |
| ICD-9-CM | 427.69 |
| DiseasesDB | 32412 |
| eMedicine | emerg/773 |
| MeSH | D018879 |
A premature ventricular contraction (PVC) — also known as a premature ventricular complex, ventricular premature contraction (or complex or complexes) (VPC), ventricular premature beat (VPB), or ventricular extrasystole (VES) — is a relatively common event where the heartbeat is initiated by Purkinje fibers in the ventricles rather than by the sinoatrial node, the normal heartbeat initiator. The electrical events of the heart detected by the electrocardiogram (ECG) allow a PVC to be easily distinguished from a normal heart beat. Although a PVC can be a sign of decreased oxygenation to the heart muscle, often PVCs are benign and may even be found in otherwise healthy hearts.[1]
A PVC may be perceived as a "skipped beat" or felt as palpitations in the chest. In a normal heartbeat, the ventricles contract after the atria have helped to fill them by contracting; in this way the ventricles can pump a maximized amount of blood both to the lungs and to the rest of the body. In a PVC, the ventricles contract first and before the atria have optimally filled the ventricles with blood, which means that circulation is inefficient. However, single beat PVC abnormal heart rhythms do not usually pose a danger and can be asymptomatic in healthy individuals.[2]
A PVC is a type of ectopic beat.
Prevalence
Single PVC are common in healthy persons. In 101 people free of heart disease during 24 hours Holter monitoring, 39 had at least 1 PVC, and 4 at least 100. Heart disease was excluded after physical examination, chest x-ray, ECG, echocardiography, maximal exercise stress test, right- and left-heart catheterization and coronary angiography. [3] In 122,043 United States Air Force flyers and cadet applicants during approximately 48 seconds of ECG 0.78% (952 males) had PVC within all age groups, but with increased incidence with increasing age. [4]
Signs and symptoms
Although there are many signs and symptoms associated with PVCs, PVCs may have no symptoms at all. An isolated PVC is hard to catch without the use of a Holter monitor. PVCs may be perceived as a skipped heart beat, a strong beat, or a feeling of suction in the chest. They may also cause chest pain, a faint feeling, fatigue, or hyperventilation after exercise.[5] Several PVCs in a row becomes a form of ventricular tachycardia (VT), which is a potentially fatal abnormal heart rhythm.
Some other possible signs and symptoms of PVCs:
- Abnormal ECG
- Irregular heart beat
- Dyspnea
- Dizziness
- Feeling your heart beat (palpitations)
- Feeling of occasional, forceful beats
- Increased awareness of your heart beat
Causes
Premature ventricular contractions can occur in a healthy person of any age, but are more prevalent in the elderly and in men.[6] They frequently occur spontaneously with no known cause. Heart rate turbulence (HRT) is a phenomenon representing the return to equilibrium of the heart rate after a PVC. HRT parameters correlate significantly with mortality after myocardial infarction (heart attack).[7] Some possible causes of PVCs include:
- Adrenaline excess;[5]
- High blood calcium;[6]
- Cardiomyopathy, hypertrophic or dilated;[6]
- Certain medicines such as digoxin, which increases heart contraction or tricyclic antidepressants[6]
- Chemical (electrolyte) problems in the blood;[8]
- Contact with Carina (trachea/bronchi) when performing medical suctioning stimulates vagus nerve
- Drugs such as:[6]
- Myocardial infarction;[5]
- Hypercapnia (CO2 poisoning);[6]
- Hypoxia;[6]
- Ischemia;[9]
- Lack of sleep/exhaustion;[12]
- Magnesium and potassium deficiency;[6]
- Mitral valve prolapse;[6]
- Myocardial contusion;[6]
- Myocarditis;[6]
- Sarcoidosis;[13]
- Smoking;[9]
- Stress;[12]
- Thyroid problems;[14]
Diagnosis
PVCs are usually diagnosed after the patient has described "skipped beats", pauses or palpitations. Typically the palpitations felt by PVC patients are very irregular and less sustained than patients with other types of arrhythmia. They are likely to have "flip flopping" sensations where it feels like the heart is flipping over or pounding due to there being a pause after the premature contraction and then a powerful contraction after the pause. There is a possibility that they might feel a ‘fluttering’ in their chest or a pounding in their neck but these two types of palpitations aren’t very common in PVC patients.[15]
A physical examination should be conducted after a full history has been taken. This is useful in determining any possible heart defects that might be causing the palpitations. For example, some cases of premature ventricular contraction have a mitral-valve prolapse which can be determined through the physical examination.[15] The next step in diagnosis is a 12 lead ECG which can be performed in the doctors’ office over a short period of time; however this is often non-conclusive in diagnosis because it is not very sensitive and there is only a small chance of a premature ventricular contraction occurring in the short period of time. Holter monitoring is a far better method for diagnosis as it is continuous recording of the heart’s rhythm over a period of 24 hours, or event monitoring which records noncontinuously for 30 days or indefinitely. This increases the likelihood of a premature ventricular contraction occurring during the recording period and is therefore more useful in diagnosis.[16] A simple self-diagnosis can be made with an inexpensive blood-oxygenation sensor/monitor that is put on a finger, displaying additionally the continuous on-going graph of the heart beating. That sensor can stay on the finger indefinitely without paying attention to it, but whenever a palpitation is being felt, a glance on the display will tell if a beat was skipped. If the problem repeats, the graph can be manually copied on a piece of paper, or - if the monitor has that feature - stored in the monitor's memory.
When looking at an electrocardiograph, premature ventricular contractions are easily spotted and therefore a definitive diagnosis can be made. The QRS and T waves look very different from normal readings. The spacing between the PVC and the preceding QRS wave is a lot shorter than usual and the time between the PVC and the proceeding QRS is a lot longer. However, the time between the preceding and proceeding QRS waves stays the same as normal due to the compensatory pause.[17] PVCs can be distinguished from premature atrial contractions because the compensatory pause is longer following premature ventricular contractions.[18]
There are four different named patterns of regularly occurring PVCs. Depending whether there are 1, 2, or 3 normal beats between each PVC, the rhythm is called bigeminy, trigeminy, or quadrigeminy. Unifocal PVCs are triggered from a single site in the ventricle, causing the peaks on the ECG to look the same. Multifocal PVCs arise when more than one site in the ventricles initiate depolarization, causing each peak on the ECG to have a different shape. If 3 or more PVCs occur in a row it may be called ventricular tachycardia.[18]
Pathophysiology
Normally, impulses pass through both ventricles almost at the same time and the depolarization waves of the two ventricles partially cancel each other out in the ECG. However, when a PVC occurs the impulse nearly always travels through only one bundle fiber, so there is no neutralization effect; this results in the high voltage QRS wave in the electrocardiograph.
There are three main physiological explanations for premature ventricular contractions: enhanced ectopic nodal automaticity, re-entry signalling, and toxic/reperfusion triggered.
Ectopic enhanced nodal automaticity suggests foci of sub-pulmonic valvular pacemaker cells that have a subthreshold potential for firing. The basic rhythm of the heart raises these cells to threshold, which precipitates an ectopic beat. This process is the underlying mechanism for arrhythmias due to excess catecholamines and some electrolyte deficiencies, particularly low blood potassium.
Reentry occurs when an area of 1-way block in the Purkinje fibers and a second area of slow conduction are present. This condition is frequently seen in patients with underlying heart disease that creates areas of differential conduction and recovery due to myocardial scarring or ischemia. During ventricular activation, one bundle tract's area of slow conduction activates the other tract's bundle fibers post block after the rest of the ventricle has recovered. This resulting in an extra beat. Reentry can produce single ectopic beats, or it can trigger paroxysmal tachycardia.
Triggered beats are considered to be due to after-depolarizations triggered by the preceding action potential. These are often seen in patients with ventricular arrhythmias due to digoxin toxicity and reperfusion therapy after myocardial infarction (MI).[6]
Molecular basis
There are a number of different molecular explanations for PVCs.
- calcium excess: One explanation is most basically due to an increased amount of cyclic AMP(cAMP) in the muscle cells of the heart's ventricles leading to increased flow of calcium ions into the cell. This may happen for the following reasons:
- Activation of the sympathetic nervous system, due to anxiety and/or physiological stress, for example hypovolemia caused by dehydration or bleeding. This activation can cause a release of catecholamines such as epinephrine (adrenaline) which can bind to beta-1 adrenergic receptor (β1 receptors) on cardiac myocytes, activating a type of guanosine nucleotide-binding protein called Gs protein.[19] This type of protein stimulates the production of cAMP,[20] ultimately increasing the flow of calcium ions from the extracellular space and from the sarcoplasmic reticulum into the cytosol.[21]
This has the effect of (1) increasing the strength of contraction (inotropy) and (2) depolarizing the myocyte more rapidly (chronotropy). The ventricular myocytes are therefore more irritable than usual, and may depolarize spontaneously before the SA node depolarizes. Other sympathomimetic molecules such as amphetamines and cocaine will also cause this effect. - Phosphodiesterase inhibitors such as caffeine directly affect the G-coupled signal transduction cascade[22] by inhibiting the enzyme that catalyzes the breakdown of cAMP,[19] again leading to the increased concentration of calcium ions in the cytosol.
- Activation of the sympathetic nervous system, due to anxiety and/or physiological stress, for example hypovolemia caused by dehydration or bleeding. This activation can cause a release of catecholamines such as epinephrine (adrenaline) which can bind to beta-1 adrenergic receptor (β1 receptors) on cardiac myocytes, activating a type of guanosine nucleotide-binding protein called Gs protein.[19] This type of protein stimulates the production of cAMP,[20] ultimately increasing the flow of calcium ions from the extracellular space and from the sarcoplasmic reticulum into the cytosol.[21]
- potassium deficiency: Potassium ion concentrations are a major determinant in the magnitude of the electrochemical potential of cells, and hypokalemia makes it more likely that cells will depolarize spontaneously. Hypercalcemia has a similar effect, although clinically it is of less concern.
- magnesium deficiency: Magnesium ions affect the flow of calcium ions, and they affect the function of the Na+/K+ ATPase, and are necessary for maintaining potassium levels. Low blood magnesium therefore also makes spontaneous depolarization more likely.
- myocardium damage: Existing damage to the myocardium can also provoke PVCs. The myocardial scarring that occurs in myocardial infarction and also in the surgical repair of congenital heart disease can disrupt the conduction system of the heart and may also irritate surrounding viable ventricular myocytes, make them more likely to depolarize spontaneously. Inflammation of the myocardium (as occurs in myocarditis) and systemic inflammation cause surges of cytokines, which can affect the electrical properties of myocytes and may be ultimately responsible for causing irritability of myocytes.
Treatment
Isolated PVCs with benign characteristics require no treatment. In healthy individuals, PVCs can often be resolved by restoring the balance of magnesium, calcium and potassium within the body. In one randomized controlled trial with 60 people those with 260 mg magnesium daily supplementation (in magnesium pidolate) had an average reduction of PVC by 77%.[23] In another trial with 232 persons with frequent ventricular arrhythmias (> 720 PVC/24 h) those with 6 mmol of magnesium (146 mg Mg)/12 mmol of potassium-DL-hydrogenaspartate daily supplementation had median reduction of PVCs by 17%.[24]
The most effective treatment is the elimination of triggers (particularly stopping the use of substances such as caffeine and certain drugs).
- Medications
- Antiarrhythmics:[6] these agents alter the electrophysiologic mechanisms responsible for PVCs. In CAST study of survivors of myocardial infarction encainide and flecainide, although could suppress PVC, they increased death risk;[25] moricizine increased death rate when used with diuretics and decreased it when used alone.[26]
- Beta blockers[5]
- Calcium channel blockers[5]
- Electrolytes replacement
- Magnesium supplements (e.g. magnesium citrate, orotate, Maalox, etc.)
- Potassium supplements (e.g. chloride potassium with citrate ion)
- Radiofrequency catheter ablation treatment.[5] It is advised for people with ventricular dysfunction and frequent arrhythmias or very frequent PVC (>20% in 24 h) and normal ventricular function.[27]
- Implantable cardioverter-defibrillator[25]
- Lifestyle modification
- Frequently stressed individuals should consider therapy, or joining a support group.
- Heart attacks can increase the likelihood of having PVCs.[5]
In the setting of existing heart disease, however, PVCs must be watched carefully, as they may cause a form of ventricular tachycardia (rapid heartbeat).
The American College of Cardiology and the American Heart Association recommend evaluation for coronary artery disease (CAD) in patients who have frequent PVCs and cardiac risk factors, such as hypertension and smoking (SOR C). Evaluation for CAD may include stress testing, echocardiography, and ambulatory rhythm monitoring.
Prognosis
In meta-analysis of 11 studies, people with frequent PVC (≥1 time during a standard electrocardiographic recording or ≥30 times over a 1-hour recording) had risk of cardiac death 2 times higher than persons without frequent PVC. Although most studies made attempts to exclude high-risk subjects, such as those with histories of cardiovascular disease, they did not test participants for underlying structural heart disease.[28]
In a study of 239 people with frequent PVCs (>1000 beats/day) and without structural heart disease (i.e. in the presence of normal heart function) there was no serious cardiac events through 5.6 years on average, but there was correlation between PVC prevalence and decrease of ejection fraction and increase of left ventricular diastolic dimension. In this study absence of heart of disease was excluded by echocardiography, cardiac magnetic resonance imaging in 63 persons and Holter monitoring.[29] Another study has suggested that in the absence of structural heart disease even frequent (> 60/h or 1/min) and complex PVCs are associated with a benign prognosis.[25] It was study of 70 people followed by 6.5 years on average. Healthy status was confirmed by extensive noninvasive cardiologic examination, although cardiac catheterization of a subgroup disclosed serious coronary artery disease in 19%. Overall survival was better than expected.[30]
On the other hand, the Framingham Heart Study reported that PVCs in apparently healthy people were associated with a twofold increase in the risk of all-cause mortality, myocardial infarction and cardiac death.[25] In men with coronary heart disease and in women with or without coronary heart disease, complex or frequent arrhythmias were not associated with an increased risk.[31] The at-risk people might have subclincal coronary disease.[32] These Framingham results have been criticised for the lack of rigorous measures to exclude the potential confounder of underlying heart disease.[25]
In the ARIC study of 14,783 people followed for 15 to 17 years those with detected PVC during 2 minute ECG, and without hypertension or diabetes on the beginning, had risk of stroke increased by 109%.[33] Hypertension or diabetes, both risk factors for stroke, did not change significantly risk of stroke for people with PVC.[33] It is possible that PVCs identified those at risk of stroke with blood pressure and impaired glucose tolerance on a continuum of risk below conventional diagnostic thresholds for hypertension and diabetes.[33] Those in ARIC study with any PVC had risk of heart failure increased by 63%[34] and were >2 times as likely to die due to coronary heart disease (CHD). Risk was also higher for people with or without baseline CHD.[35]
In the Niigata study of 63,386 people with 10-year follow-up period those with PVC during a 10-second recording had risk of atrial fibrillation increased nearly 3 times independently from risk factors: age, male sex, body mass index, hypertension, systolic and diastolic blood pressure, and diabetes.[36]
Reducing frequent PVC (>20%) by antiarrhythmic drugs or by catheter ablation significantly improves heart performance.[25][27]
Recent studies have shown that those subjects who have an extremely high occurrence of PVCs (several thousand a day) can develop dilated cardiomyopathy. In these cases, if the PVCs are reduced or removed (for example, via ablation therapy) the cardiomyopathy usually regresses.[27][37]
Also, PVCs can permanently cease without any treatment, in a material percentage of cases.
See also
References
- ↑ What is a PVC
- ↑ Stanfield, C.; Germann, W. (2008), Principles of Human Physiology (3rd ed.), Pearson International Edition, p. 378, ISBN 0-321-45506-1
- ↑ Kostis, J. B.; McCrone, K.; Moreyra, A. E.; Gotzoyannis, S.; Aglitz, N. M.; Natarajan, N.; Kuo, P. T. (1 June 1981). "Premature ventricular complexes in the absence of identifiable heart disease". Circulation. 63 (6): 1351–1356. doi:10.1161/01.CIR.63.6.1351.
- ↑ Hiss, R. G.; Lamb, L. E. (1 June 1962). "Electrocardiographic Findings in 122,043 Individuals". Circulation. 25 (6): 947–961. doi:10.1161/01.CIR.25.6.947. PMID 13907778.
- 1 2 3 4 5 6 7 http://www.uptodate.com/patients/content/topic.do?topicKey=hrt_dis/11733, Up-to-date
- 1 2 3 4 5 6 7 8 9 10 11 12 13 Premature ventricular contraction at eMedicine
- ↑ Francis J, Watanabe MA, Schmidt G (January 2005), "Heart rate turbulence: a new predictor for risk of sudden cardiac death.", Ann. Noninvasive Electrocardiol., 10: 102–9, doi:10.1111/j.1542-474X.2005.10102.x, PMID 15649245
- ↑ MedlinePlus Encyclopedia Ectopic heartbeat
- 1 2 3 Emilsson K (June 2008), "Suspected association of ventricular arrhythmia with air pollution in a motorbike rider: a case report", J Med Case Reports, 2: 192, doi:10.1186/1752-1947-2-192, PMC 2427047
 , PMID 18522736
, PMID 18522736 - ↑ "Premature ventricular contractions (PVCs) Causes". Diseases and Conditions. Mayo Clinic.
- ↑ Lebowitz, Dr. Michael. "Methylxanthine Toxcity Syndrome". Retrieved 25 January 2016.
- 1 2 Guyton MD, Arthur C.; Hall, John E. (2006). Textbook of medical physiology (11th ed.). p. 151. ISBN 0-7216-0240-1.
- ↑ Birnie D, "HRS Expert Consensus Statement on the Diagnosis and Management of Arrhythmias Associated With Cardiac Sarcoidosis", Heart Rhythm, 11: 1304, doi:10.1016/j.hrthm.2014.03.043
- ↑ "Premature Ventricular Contractions". HealthCentral.
- 1 2 Zimetbaum P, Josephson ME (1998). "Evaluation of patients with palpitations". N. Engl. J. Med. 338 (19): 1369–73. doi:10.1056/NEJM199805073381907. PMID 9571258.
- ↑ Meurs KM, Spier AW, Wright NA, Hamlin RL (January 2001). "Comparison of in-hospital versus 24-hour ambulatory electrocardiography for detection of ventricular premature complexes in mature Boxers". J. Am. Vet. Med. Assoc. 218 (2): 222–4. doi:10.2460/javma.2001.218.222. PMID 11195827.
- ↑ Levy 2007, pp. 49–50
- 1 2 Haist, Steven A.; Gomella, Leonard G. (2004), "19 Basic ECG Reading: Ventricular Arrhythmias", Clinician's pocket reference (10th ed.), New York: McGraw-Hill, p. 390, ISBN 0-07-140255-1
- 1 2 Nelson 2008, p. 424
- ↑ Levy 2007, p. 62
- ↑ Levy 2007, p. 24
- ↑ Nelson 2008, p. 430
- ↑ Falco, CN; Grupi, C; Sosa, E; Scanavacca, M; Hachul, D; Lara, S; Sacilotto, L; Pisani, CF; Ramires, JA; Darrieux, F (June 2012). "Successful improvement of frequency and symptoms of premature complexes after oral magnesium administration.". Arquivos brasileiros de cardiologia. 98 (6): 480–7. PMID 22584491.
- ↑ Zehender, M; Meinertz, T; Faber, T; Caspary, A; Jeron, A; Bremm, K; Just, H (April 1997). "Antiarrhythmic effects of increasing the daily intake of magnesium and potassium in patients with frequent ventricular arrhythmias. Magnesium in Cardiac Arrhythmias (MAGICA) Investigators.". Journal of the American College of Cardiology. 29 (5): 1028–34. doi:10.1016/s0735-1097(97)00053-3. PMID 9120155.
- 1 2 3 4 5 6 G André Ng (2006). "Treating patients with ventricular ectopic beats". Heart. 92 (11): 1707–12. doi:10.1136/hrt.2005.067843. PMC 1861260. PMID 17041126.
- ↑ Anderson, JL; Platia, EV; Hallstrom, A; Henthorn, RW; Buckingham, TA; Carlson, MD; Carson, PE (December 1994). "Interaction of baseline characteristics with the hazard of encainide, flecainide, and moricizine therapy in patients with myocardial infarction. A possible explanation for increased mortality in the Cardiac Arrhythmia Suppression Trial (CAST).". Circulation. 90 (6): 2843–52. doi:10.1161/01.cir.90.6.2843. PMID 7994829.
- 1 2 3 Belhassen B (2005). "Radiofrequency ablation of "benign" right ventricular outflow tract extrasystoles: a therapy that has found its disease?". J. Am. Coll. Cardiol. 45 (8): 1266–8. doi:10.1016/j.jacc.2005.01.028. PMID 15837260.
- ↑ Ataklte, F; Erqou, S; Laukkanen, J; Kaptoge, S (15 October 2013). "Meta-analysis of ventricular premature complexes and their relation to cardiac mortality in general populations.". The American journal of cardiology. 112 (8): 1263–70. doi:10.1016/j.amjcard.2013.05.065. PMID 23927786.
- ↑ Niwano, S; Wakisaka, Y; Niwano, H; Fukaya, H; Kurokawa, S; Kiryu, M; Hatakeyama, Y; Izumi, T (August 2009). "Prognostic significance of frequent premature ventricular contractions originating from the ventricular outflow tract in patients with normal left ventricular function.". Heart (British Cardiac Society). 95 (15): 1230–7. doi:10.1136/hrt.2008.159558. PMID 19429571.
- ↑ Kennedy, HL; Whitlock, JA; Sprague, MK; Kennedy, LJ; Buckingham, TA; Goldberg, RJ (24 January 1985). "Long-term follow-up of asymptomatic healthy subjects with frequent and complex ventricular ectopy.". The New England Journal of Medicine. 312 (4): 193–7. doi:10.1056/nejm198501243120401. PMID 2578212.
- ↑ Bikkina, M; Larson, MG; Levy, D (15 December 1992). "Prognostic implications of asymptomatic ventricular arrhythmias: the Framingham Heart Study.". Annals of Internal Medicine. 117 (12): 990–6. doi:10.7326/0003-4819-117-12-990. PMID 1280018.
- ↑ Moss, AJ (15 December 1992). "Asymptomatic ventricular arrhythmias in healthy persons: smoke or smoke screen?". Annals of Internal Medicine. 117 (12): 1053–4. doi:10.7326/0003-4819-117-12-1053. PMID 1443975.
- 1 2 3 Worthington, JM; Gattellari, M; Leung, DY (April 2010). "'Where there's smoke ...': are premature ventricular complexes a new risk factor for stroke?". Stroke; a journal of cerebral circulation. 41 (4): 572–3. doi:10.1161/strokeaha.109.574426. PMID 20167909.
- ↑ Agarwal, SK; Simpson RJ, Jr; Rautaharju, P; Alonso, A; Shahar, E; Massing, M; Saba, S; Heiss, G (1 January 2012). "Relation of ventricular premature complexes to heart failure (from the Atherosclerosis Risk In Communities [ARIC] Study).". The American journal of cardiology. 109 (1): 105–9. doi:10.1016/j.amjcard.2011.08.009. PMID 21945138.
- ↑ Massing, MW; Simpson RJ, Jr; Rautaharju, PM; Schreiner, PJ; Crow, R; Heiss, G (15 December 2006). "Usefulness of ventricular premature complexes to predict coronary heart disease events and mortality (from the Atherosclerosis Risk In Communities cohort).". The American journal of cardiology. 98 (12): 1609–12. doi:10.1016/j.amjcard.2006.06.061. PMID 17145219.
- ↑ Watanabe, H; Tanabe, N; Makiyama, Y; Chopra, SS; Okura, Y; Suzuki, H; Matsui, K; Watanabe, T; Kurashina, Y; Aizawa, Y (October 2006). "ST-segment abnormalities and premature complexes are predictors of new-onset atrial fibrillation: the Niigata preventive medicine study.". American Heart Journal. 152 (4): 731–5. doi:10.1016/j.ahj.2006.05.032. PMID 16996849.
- ↑ Shiraishi H, Ishibashi K, Urao N, Tsukamoto M, Hyogo M, Keira N, Hirasaki S, Shirayama T, Nakagawa M (2002). "A case of cardiomyopathy induced by premature ventricular complexes". Circ. J. 66 (11): 1065–7. doi:10.1253/circj.66.1065. PMID 12419942.
Further reading
- Levy, M.N.; Pappano, A.J. (2007). Cardiovascular physiology (9th ed.). Mosby Elsevier. ISBN 0-323-03446-2.
- Nelson, D.L.; Cox, M.M. (2008). Lehninger Principles of Biochemistry (5th ed.). WH Freeman. ISBN 0-7167-7108-X.