Tetrahydrocannabinol
 | |
 | |
| Clinical data | |
|---|---|
| Trade names | Marinol |
| License data |
|
| Pregnancy category |
|
| Dependence liability | 8–10% (Relatively low risk of tolerance)[1] |
| Addiction liability | Low |
| Routes of administration | Orally, local/topical, transdermal, sublingual, inhaled |
| ATC code | A04AD10 (WHO) |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | 10–35% (inhalation), 6–20% (oral)[3] |
| Protein binding | 97–99%[3][4][5] |
| Metabolism | Mostly hepatic by CYP2C[3] |
| Biological half-life | 1.6–59 h,[3] 25–36 h (orally administered dronabinol) |
| Excretion | 65–80% (feces), 20–35% (urine) as acid metabolites[3] |
| Identifiers | |
| |
| Synonyms | (6aR,10aR)-delta-9-tetrahydrocannabinol |
| CAS Number |
1972-08-3 |
| PubChem (CID) | 16078 |
| IUPHAR/BPS | 2424 |
| DrugBank |
DB00470 |
| ChemSpider |
15266 |
| UNII |
7J8897W37S |
| ChEBI |
CHEBI:66964 |
| ChEMBL |
CHEMBL465 |
| ECHA InfoCard | 100.153.676 |
| Chemical and physical data | |
| Formula | C21H30O2 |
| Molar mass | 314.469 g/mol |
| 3D model (Jmol) | Interactive image |
| Specific rotation | −152° (ethanol) |
| Boiling point | 157 °C (315 °F) [6] |
| Solubility in water | 0.0028,[7] (23 °C) mg/mL (20 °C) |
| |
| |
| | |
Tetrahydrocannabinol (THC, dronabinol by INN), or more precisely its main isomer (−)-trans-Δ9-tetrahydrocannabinol, is the principal psychoactive constituent (or cannabinoid) of cannabis. It can be an amber or gold colored glassy solid when cold, which becomes viscous and sticky if warmed.
Like most pharmacologically-active secondary metabolites of plants, THC in Cannabis is assumed to be involved in self-defense, perhaps against herbivores.[8] THC also possesses high UV-B (280–315 nm) absorption properties, which, it has been speculated, could protect the plant from harmful UV radiation exposure.[9][10][11]
THC, along with its double bond isomers and their stereoisomers, is one of only three cannabinoids scheduled by the UN Convention on Psychotropic Substances (the other two are dimethylheptylpyran and parahexyl). It was listed under Schedule I in 1971, but reclassified to Schedule II in 1991 following a recommendation from the WHO. Based on subsequent studies, the WHO has recommended the reclassification to the less-stringent Schedule III.[12] Cannabis as a plant is scheduled by the Single Convention on Narcotic Drugs (Schedule I and IV).
A pharmaceutical formulation is available by prescription in the U.S. and Canada under the brand name Marinol.
Medical uses
Dronabinol is the INN for a pure isomer of THC, (–)-trans-Δ9-tetrahydrocannabinol,[13] which is the main isomer found in cannabis. It is used to treat anorexia in people with HIV/AIDS as well as for refractory nausea and vomiting in people undergoing chemotherapy. It is safe and effective for these uses.[14][15]
THC is also an active ingredient in nabiximols, a specific extract of Cannabis that was approved as a botanical drug in the United Kingdom in 2010 as a mouth spray for people with multiple sclerosis to alleviate neuropathic pain, spasticity, overactive bladder, and other symptoms.[16][17]
Adverse effects


Acute toxicity
There has never been a documented human fatality solely from overdosing on tetrahydrocannabinol.[18] However, numerous reports have suggested an association of cannabis smoking with an increased risk of myocardial infarction (heart attack);[19][20] however, oral administration does not have this effect. Information about the toxicity of THC is primarily based on results from non-human studies. The toxicity depends on the route of administration and the laboratory animal.
An overdose of dronabinol usually presents with lethargy, decreased motor coordination, slurred speech, and postural hypotension. The FDA estimates the lethal human dose of intravenous dronabinol to be 30 mg/kg (2100 mg/ 70 kg).[21] The typical medicinal dosage administered is two 2.5 mg capsules daily for an 80 kg man (~170 lb). A lethal dose for such a person would be approximately 960 of those capsules infused intravenously. Non-fatal overdoses have occurred: "Significant CNS symptoms in antiemetic studies followed oral doses of 0.4 mg/kg (28 mg/70 kg) of dronabinol capsules."[22]
A meta analysis of clinical trials conducted using standardized cannabis extracts or THC conducted by the American Academy of Neurology found that of 1619 persons treated with cannabis products (including some treated with smoked cannabis and nabiximols), 6.9% discontinued due to side effects, compared to 2.2% of 1,118 treated with placebo. Detailed information regarding side effects was not available from all trials, but nausea, increased weakness, behavioral or mood changes, suicidal ideation, hallucinations, dizziness, and vasovagal symptoms, fatigue, and feelings of intoxication were each described as side effects in at least two trials. There was a single death rated by the investigator as "possibly related" to treatment. This person had a seizure followed by aspiration pneumonia. The paper does not describe whether this was one of the subjects from the epilepsy trials.[23]
Pharmacology
Mechanism of action
The actions of THC result from its partial agonist activity at the cannabinoid receptor CB1 (Ki=10nM[24]), located mainly in the central nervous system, and the CB2 receptor (Ki=24nM[24]), mainly expressed in cells of the immune system.[25] The psychoactive effects of THC are primarily mediated by its activation of CB1G-protein coupled receptors, which result in a decrease in the concentration of the second messenger molecule cAMP through inhibition of adenylate cyclase.[26]
The presence of these specialized cannabinoid receptors in the brain led researchers to the discovery of endocannabinoids, such as anandamide and 2-arachidonoyl glyceride (2-AG). THC targets receptors in a manner far less selective than endocannabinoid molecules released during retrograde signaling, as the drug has a relatively low cannabinoid receptor efficacy and affinity. In populations of low cannabinoid receptor density, THC may act to antagonize endogenous agonists that possess greater receptor efficacy.[27] THC is a lipophilic molecule[28] and may bind non-specifically to a variety of entities in the brain and body, such as adipose tissue (fat).[29][30]
THC, similarly to cannabidiol, albeit less potently, is a positive allosteric modulator of the μ- and δ-opioid receptors.[31]
Due to its partial agonistic activity, THC appears to result in greater downregulation of cannabinoid receptors than endocannabinoids, further limiting its efficacy over other cannabinoids. While tolerance may limit the maximal effects of certain drugs, evidence suggests that tolerance develops irregularly for different effects with greater resistance for primary over side-effects, and may actually serve to enhance the drug's therapeutic window.[27] However, this form of tolerance appears to be irregular throughout mouse brain areas. THC, as well as other cannabinoids that contain a phenol group, possesses mild antioxidant activity sufficient to protect neurons against oxidative stress, such as that produced by glutamate-induced excitotoxicity.[25]
Pharmacokinetics
THC is metabolized mainly to 11-OH-THC by the body. This metabolite is still psychoactive and is further oxidized to 11-nor-9-carboxy-THC (THC-COOH). In humans and animals, more than 100 metabolites could be identified, but 11-OH-THC and THC-COOH are the dominating metabolites.[32] Metabolism occurs mainly in the liver by cytochrome P450 enzymes CYP2C9, CYP2C19, and CYP3A4.[33] More than 55% of THC is excreted in the feces and ~20% in the urine. The main metabolite in urine is the ester of glucuronic acid and THC-COOH and free THC-COOH. In the feces, mainly 11-OH-THC was detected.[34]
Physical and chemical properties
Discovery and structure identification
The discovery of THC, by a team of researchers from Hebrew University Pharmacy School, was first reported in 1964,[35] with substantial later work reported by Raphael Mechoulam in June 1970.[36]
Solubility
An aromatic terpenoid, THC has a very low solubility in water, but good solubility in most organic solvents, specifically lipids and alcohols.[7] THC, CBD, CBN, CBC, CBG and over 113 other molecules make up the phytocannabinoid family.[37][38]
Biosynthesis
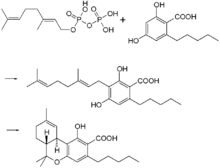
In the Cannabis plant, THC occurs mainly as tetrahydrocannabinolic acid (THCA, 2-COOH-THC, THC-COOH). Geranyl pyrophosphate and olivetolic acid react, catalysed by an enzyme to produce cannabigerolic acid,[39] which is cyclized by the enzyme THC acid synthase to give THCA. Over time, or when heated, THCA is decarboxylated, producing THC. The pathway for THCA biosynthesis is similar to that which produces the bitter acid humulone in hops.[40][41]
Detection in body fluids
THC, 11-OH-THC and THC-COOH can be detected and quantified in blood, urine, hair, oral fluid or sweat using a combination of immunoassay and chromatographic techniques as part of a drug use testing program or in a forensic investigation.[42][43][44]
History
THC was first isolated in 1964 by Raphael Mechoulam and Yechiel Gaoni at the Weizmann Institute of Science.[35][45][46]
Since at least 1986, the trend has been for THC in general, and especially the Marinol preparation, to be downgraded to less and less stringently-controlled schedules of controlled substances, in the U.S. and throughout the rest of the world.
On May 13, 1986, the Drug Enforcement Administration (DEA) issued a Final Rule and Statement of Policy authorizing the "Rescheduling of Synthetic Dronabinol in Sesame Oil and Encapsulated in Soft Gelatin Capsules From Schedule I to Schedule II" (DEA 51 FR 17476-78). This permitted medical use of Marinol, albeit with the severe restrictions associated with Schedule II status.[47] For instance, refills of Marinol prescriptions were not permitted. At its 1045th meeting, on April 29, 1991, the Commission on Narcotic Drugs, in accordance with article 2, paragraphs 5 and 6, of the Convention on Psychotropic Substances, decided that Δ9-tetrahydrocannabinol (also referred to as Δ9-THC) and its stereochemical variants should be transferred from Schedule I to Schedule II of that Convention. This released Marinol from the restrictions imposed by Article 7 of the Convention (See also United Nations Convention Against Illicit Traffic in Narcotic Drugs and Psychotropic Substances).
An article published in the April–June 1998 issue of the Journal of Psychoactive Drugs found that "Healthcare professionals have detected no indication of scrip-chasing or doctor-shopping among the patients for whom they have prescribed dronabinol". The authors state that Marinol has a low potential for abuse.[48]
In 1999, Marinol was rescheduled from Schedule II to III of the Controlled Substances Act, reflecting a finding that THC had a potential for abuse less than that of cocaine and heroin. This rescheduling constituted part of the argument for a 2002 petition for removal of cannabis from Schedule I of the Controlled Substances Act, in which petitioner Jon Gettman noted, "Cannabis is a natural source of dronabinol (THC), the ingredient of Marinol, a Schedule III drug. There are no grounds to schedule cannabis in a more restrictive schedule than Marinol".[49]
At its 33rd meeting, in 2003, the World Health Organization Expert Committee on Drug Dependence recommended transferring THC to Schedule IV of the Convention, citing its medical uses and low abuse potential.[50]
Society and culture
Brand names
Dronabinol is marketed as Marinol,[51] a registered trademark of Solvay Pharmaceuticals. Dronabinol is also marketed, sold, and distributed by PAR Pharmaceutical Companies under the terms of a license and distribution agreement with SVC pharma LP, an affiliate of Rhodes Technologies. Dronabinol is available as a prescription drug (under Marinol[52]) in several countries including the United States, Germany, South Africa and Australia.[53] In the United States, Marinol is a Schedule III drug, available by prescription, considered to be non-narcotic and to have a low risk of physical or mental dependence. Efforts to get cannabis rescheduled as analogous to Marinol have not succeeded thus far, though a 2002 petition has been accepted by the DEA. As a result of the rescheduling of Marinol from Schedule II to Schedule III, refills are now permitted for this substance. Marinol's U.S. Food and Drug Administration (FDA) approvals for medical use has raised much controversy[54] as to why natural THC is considered a schedule I drug.[55]
Comparisons with medical cannabis

Female cannabis plants contain at least 113 cannabinoids,[56] including cannabidiol (CBD), thought to be the major anticonvulsant that helps people with multiple sclerosis;[57] and cannabichromene (CBC), an anti-inflammatory which may contribute to the pain-killing effect of cannabis.[58]
It takes over one hour for Marinol to reach full systemic effect,[59] compared to seconds or minutes for smoked or vaporized cannabis.[60] Some people accustomed to inhaling just enough cannabis smoke to manage symptoms have complained of too-intense intoxication from Marinol's predetermined dosages. Many people using Marinol have said that Marinol produces a more acute psychedelic effect than cannabis, and it has been speculated that this disparity can be explained by the moderating effect of the many non-THC cannabinoids present in cannabis. For that reason, alternative THC-containing medications based on botanical extracts of the cannabis plant such as nabiximols are being developed. Mark Kleiman, director of the Drug Policy Analysis Program at UCLA's School of Public Affairs said of Marinol, "It wasn't any fun and made the user feel bad, so it could be approved without any fear that it would penetrate the recreational market, and then used as a club with which to beat back the advocates of whole cannabis as a medicine."[61] Mr. Kleiman's opinion notwithstanding, clinical trials comparing the use of cannabis extracts with Marinol in the treatment of cancer cachexia have demonstrated equal efficacy and well-being among subjects in the two treatment arms.[62] United States federal law currently registers dronabinol as a Schedule III controlled substance, but all other cannabinoids remain Schedule I, except synthetics like nabilone.[63]
Research
Its status as an illegal drug in most countries can make research difficult; for instance in the United States where the National Institute on Drug Abuse was the only legal source of cannabis for researchers until it recently became legalized in Colorado, Washington state, Oregon, Alaska, and Washington D.C.[64]
In April 2014 the American Academy of Neurology published a systematic review of the efficacy and safety of medical marijuana and marijuana-derived products in certain neurological disorders.[23] The review identified 34 studies meeting inclusion criteria, of which 8 were rated as Class I quality.[23] The study found evidence supporting the effectiveness of the cannabis extracts that were tested and THC in treating certain symptoms of multiple sclerosis, but found insufficient evidence to determine the effectiveness of the tested cannabis products in treating several other neurological diseases.[23]
Several of the clinical trials exploring the safety and efficacy of "oral cannabis extract" that were reviewed by the AAN were conducted using "Cannador", made by the Institute for Clinical Research (IKF) in Berlin,[65] which is a capsule with a standardized Cannabis sativa extract; the cannabis grown in Switzerland and processed in Germany.[66]:88 Each capsule of Cannador contains 2.5 mg Δ9- tetrahydrocannabinol and cannabidiols are standardized to a range 0.8–1.8 mg.[67]
Multiple sclerosis symptoms
- Spasticity. Based on the results of 3 high quality trials and 5 of lower quality, oral cannabis extract was rated as effective, and THC as probably effective, for improving people's subjective experience of spasticity. Oral cannabis extract and THC both were rated as possibly effective for improving objective measures of spasticity.[23]
- Centrally mediated pain and painful spasms. Based on the results of 4 high quality trials and 4 low quality trials, oral cannabis extract was rated as effective, and THC as probably effective in treating central pain and painful spasms.[23]
- Bladder dysfunction. Based on a single high quality study, oral cannabis extract and THC were rated as probably ineffective for controlling bladder complaints in multiple sclerosis[23]
Neurodegenerative disorders
- Huntington disease. No reliable conclusions could be drawn regarding the effectiveness of THC or oral cannabis extract in treating the symptoms of Huntington disease as the available trials were too small to reliably detect any difference[23]
- Parkinson disease. Based on a single study, oral cannabis extract was rated probably ineffective in treating levodopa-induced dyskinesia in Parkinson disease.[23]
- Alzheimer's disease. A 2011 Cochrane Review found insufficient evidence to conclude whether cannabis products have any utility in the treatment of Alzheimer's disease.[68]
Other neurological disorders
- Tourette syndrome. The available data was determined to be insufficient to allow reliable conclusions to be drawn regarding the effectiveness of oral cannabis extract or THC in controlling tics.[23]
- Cervical dystonia. Insufficient data was available to assess the effectiveness of oral cannabis extract of THC in treating cervical dystonia.[23]
- Epilepsy. Data was considered insufficient to judge the utility of cannabis products in reducing seizure frequency or severity.[23]
See also
- Cannabinoids
- 11-Hydroxy-THC, metabolite of THC
- Anandamide, 2-Arachidonoylglycerol, endogenous cannabinoid agonists
- Cannabidiol (CBD), an isomer of THC
- Cannabinol (CBN), a metabolite of THC
- Dimethylheptylpyran
- Parahexyl
- Tetrahydrocannabinolic acid, the biosynthetic precursor for THC
- HU-210, WIN 55,212-2, JWH-133, synthetic cannabinoid agonists
- Medical cannabis
- Nabilone
- War on Drugs
- Effects of cannabis
References
- ↑ Marlowe, Douglas B (December 2010). "The Facts On Marijuana". NADCP.
Based upon several nationwide epidemiological studies, marijuana’s dependence liability has been reliably determined to be 8 to 10 percent.
- ↑ http://www.fda.gov/ohrms/dockets/dockets/05n0479/05N-0479-emc0004-04.pdf
- 1 2 3 4 5 Grotenhermen, F (2003). "Pharmacokinetics and pharmacodynamics of cannabinoids". Clin Pharmacokinet. 42 (4): 327–60. doi:10.2165/00003088-200342040-00003. PMID 12648025. (subscription required (help)).
- ↑ The Royal Pharmaceutical Society of Great Britain (30 November 2006). "Cannabis". In Sean C. Sweetman. Martindale: The Complete Drug Reference: Single User (35th ed.). Pharmaceutical Press. ISBN 978-0-85369-703-9.
- ↑ "Tetrahydrocannabinol – Compound Summary". National Center for Biotechnology Information. PubChem. Retrieved 12 January 2014.
Dronabinol has a large apparent volume of distribution, approximately 10 L/kg, because of its lipid solubility. The plasma protein binding of dronabinol and its metabolites is approximately 97%.
- ↑ McPartland JM, Russo EB (2001). "Cannabis and cannabis extracts: greater than the sum of their parts?" (PDF). Journal of Cannabis Therapeutics. 1 (3/4): 103–132. doi:10.1300/J175v01n03_08.
- 1 2 Garrett ER, Hunt CA (July 1974). "Physicochemical properties, solubility, and protein binding of Δ9-tetrahydrocannabinol". J. Pharm. Sci. 63 (7): 1056–64. doi:10.1002/jps.2600630705. PMID 4853640.
- ↑ Pate, David W. (1994). "Chemical ecology of Cannabis". Journal of the International Hemp Association. 1 (29): 32–37.
- ↑ Pate, David W. (1983). "Possible role of ultraviolet radiation in evolution of Cannabis chemotypes". Economic Botany. 37 (4): 396–405. doi:10.1007/BF02904200.
- ↑ Lydon, John; Teramura, Alan H. (1987). "Photochemical decomposition of cannabidiol in its resin base". Phytochemistry. 26 (4): 1216–1217. doi:10.1016/S0031-9422(00)82388-2.
- ↑ Lydon J, Teramura AH, Coffman CB (1987). "UV-B radiation effects on photosynthesis, growth and cannabinoid production of two Cannabis sativa chemotypes". Photochemistry and Photobiology. 46 (2): 201–206. doi:10.1111/j.1751-1097.1987.tb04757.x. PMID 3628508.
- ↑ A Primer on the UN Drug Control Conventions. Transnational Institute
- ↑ "List of psychotropic substances under international control" (PDF). International Narcotics Control Board. p. 5. Archived from the original (PDF) on 7 September 2005. Retrieved 20 April 2011.
This international non-proprietary name refers to only one of the stereochemical variants of delta-9-tetrahydrocannabinol, namely (−)-trans-delta-9-tetrahydrocannabinol
- ↑ "Cannabis and Cannabinoids". National Cancer Institute. Retrieved 12 January 2014.
- ↑ Haney M, Gunderson EW, Rabkin J, Hart CL, Vosburg SK, Comer SD, Foltin RW (2007). "Dronabinol and marijuana in HIV-positive marijuana smokers. Caloric intake, mood, and sleep". Journal of Acquired Immune Deficiency Syndromes. 45 (5): 545–54. doi:10.1097/QAI.0b013e31811ed205. PMID 17589370.
- ↑ UK Medicines Online Nabiximols Page accessed Feb 3, 2016
- ↑ Multiple Sclerosis Trust. October 2014 Sativex (nabiximols) - factsheet
- ↑ Walker JM, Huang SM (August 2002). "Cannabinoid analgesia". Pharmacol. Ther. 95 (2): 127–35. doi:10.1016/S0163-7258(02)00252-8. PMID 12182960.
...to date, there are no deaths known to have resulted from overdose of cannabis. (p. 128)
- ↑ Thomas G, Kloner RA, Rezkalla S (January 2014). "Adverse cardiovascular, cerebrovascular, and peripheral vascular effects of marijuana inhalation: what cardiologists need to know". Am. J. Cardiol. 113 (1): 187–90. doi:10.1016/j.amjcard.2013.09.042. PMID 24176069.
- ↑ Aryana A, Williams MA (May 2007). "Marijuana as a trigger of cardiovascular events: speculation or scientific certainty?". Int. J. Cardiol. 118 (2): 141–4. doi:10.1016/j.ijcard.2006.08.001. PMID 17005273.
- ↑ "Marinol" (PDF). FDA.gov. Retrieved 14 March 2014.
- ↑ "DRONABINOL capsule [American Health Packaging]". National Library of Medicine. Daily Med. July 2012. Retrieved 12 January 2014.
The estimated lethal human dose of intravenous dronabinol is 30 mg/kg (2100 mg/70 kg). Significant CNS symptoms in antiemetic studies followed oral doses of 0.4 mg/kg (28 mg/70 kg) of dronabinol capsules.
- 1 2 3 4 5 6 7 8 9 10 11 12 Koppel BS, Brust JC, Fife T, Bronstein J, Youssof S, Gronseth G, Gloss D (April 2014). "Systematic review: Efficacy and safety of medical marijuana in selected neurologic disorders: Report of the Guideline Development Subcommittee of the American Academy of Neurology". Neurology. 82 (17): 1556–63. doi:10.1212/WNL.0000000000000363. PMC 4011465
 . PMID 24778283.
. PMID 24778283. - 1 2 "PDSP Database – UNC". NIMH Psychoactive Drug Screening Program. Retrieved 11 June 2013.
- 1 2 Pertwee RG (2006). "The pharmacology of cannabinoid receptors and their ligands: An overview". International Journal of Obesity. 30: S13–S18. doi:10.1038/sj.ijo.0803272. PMID 16570099.
- ↑ Elphick MR, Egertová M (2001). "The neurobiology and evolution of cannabinoid signalling". Philosophical Transactions of the Royal Society B: Biological Sciences. 356 (1407): 381–408. doi:10.1098/rstb.2000.0787. PMC 1088434. PMID 11316486.
- 1 2 Pertwee RG (2008). "The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: Δ9-tetrahydrocannabinol, cannabidiol and Δ9-tetrahydrocannabivarin". British Journal of Pharmacology. 153 (2): 199–215. doi:10.1038/sj.bjp.0707442. PMC 2219532. PMID 17828291.
- ↑ Rashidi H, Akhtar MT, van der Kooy F, Verpoorte R, Duetz WA (November 2009). "Hydroxylation and Further Oxidation of Δ9-Tetrahydrocannabinol by Alkane-Degrading Bacteria" (PDF). Appl Environ Microbiol. 75 (22): 7135–7141. doi:10.1128/AEM.01277-09. PMC 2786519. PMID 19767471.
Δ9-THC and many of its derivatives are highly lipophilic and poorly water soluble. Calculations of the n-octanol/water partition coefficient (Ko/w) of Δ9-THC at neutral pH vary between 6,000, using the shake flask method, and 9.44 × 106, by reverse-phase high-performance liquid chromatography estimation.
- ↑ Ashton CH (February 2001). "Pharmacology and effects of cannabis: a brief review". Br J Psychiatry. 178 (2): 101–106. doi:10.1192/bjp.178.2.101. PMID 11157422.
Because they are extremely lipid soluble, cannabinoids accumulate in fatty tissues, reaching peak concentrations in 4–5 days. They are then slowly released back into other body compartments, including the brain. ... Within the brain, THC and other cannabinoids are differentially distributed. High concentrations are reached in neocortical, limbic, sensory and motor areas.
- ↑ Huestis MA (August 2007). "Human cannabinoid pharmacokinetics". Chem Biodivers. 4 (8): 1770–804. doi:10.1002/cbdv.200790152. PMC 2689518. PMID 17712819.
THC is highly lipophilic and initially taken up by tissues that are highly perfused, such as the lung, heart, brain, and liver.
- ↑ Kathmann M, Flau K, Redmer A, Tränkle C, Schlicker E (February 2006). "Cannabidiol is an allosteric modulator at mu- and delta-opioid receptors". Naunyn Schmiedebergs Arch. Pharmacol. 372 (5): 354–61. doi:10.1007/s00210-006-0033-x. PMID 16489449.
- ↑ Aizpurua-Olaizola, Oier; Zarandona, Iratxe; Ortiz, Laura; Navarro, Patricia; Etxebarria, Nestor; Usobiaga, Aresatz (2016-01-01). "Simultaneous quantification of major cannabinoids and metabolites in human urine and plasma by HPLC-MS/MS and enzyme-alkaline hydrolysis". Drug Testing and Analysis: n/a–n/a. doi:10.1002/dta.1998. ISSN 1942-7611.
- ↑ Watanabe K, Yamaori S, Funahashi T, Kimura T, Yamamoto I (March 2007). "Cytochrome P450 enzymes involved in the metabolism of tetrahydrocannabinols and cannabinol by human hepatic microsomes". Life Science. 80 (15): 1415–9. doi:10.1016/j.lfs.2006.12.032. PMID 17303175.
- ↑ Huestis MA (2005). "Pharmacokinetics and Metabolism of the Plant Cannabinoids, Δ9-Tetrahydrocannabinol, Cannabidiol and Cannabinol". Cannabinoids. Handbook of Experimental Pharmacology. 168 (168): 657–90. doi:10.1007/3-540-26573-2_23. ISBN 3-540-22565-X. PMID 16596792.
- 1 2 Gaoni Y, Mechoulam R (1964). "Isolation, structure and partial synthesis of an active constituent of hashish". Journal of the American Chemical Society. 86 (8): 1646–1647. doi:10.1021/ja01062a046.
- ↑ Mechoulam R (1970). "Marihuana chemistry". Science. 168 (3936): 1159–66. Bibcode:1970Sci...168.1159M. doi:10.1126/science.168.3936.1159. PMID 4910003.
- ↑ El-Alfy, Abir T.; Ivey, Kelly; Robinson, Keisha; Ahmed, Safwat; Radwan, Mohamed; Slade, Desmond; Khan, Ikhlas; ElSohly, Mahmoud; Ross, Samir (2010-06-01). "Antidepressant-like effect of Δ9-tetrahydrocannabinol and other cannabinoids isolated from Cannabis sativa L". Pharmacology, biochemistry, and behavior. 95 (4): 434–442. doi:10.1016/j.pbb.2010.03.004. ISSN 0091-3057. PMC 2866040. PMID 20332000.
- ↑ Aizpurua-Olaizola, Oier; Soydaner, Umut; Öztürk, Ekin; Schibano, Daniele; Simsir, Yilmaz; Navarro, Patricia; Etxebarria, Nestor; Usobiaga, Aresatz (2016-02-02). "Evolution of the Cannabinoid and Terpene Content during the Growth ofCannabis sativaPlants from Different Chemotypes". Journal of Natural Products. 79 (2): 324–331. doi:10.1021/acs.jnatprod.5b00949.
- ↑ Fellermeier M, Zenk MH (1998). "Prenylation of olivetolate by a hemp transferase yields cannabigerolic acid, the precursor of tetrahydrocannabinol". FEBS Letters. 427 (2): 283–5. doi:10.1016/S0014-5793(98)00450-5. PMID 9607329.
- ↑ Marks MD, Tian L, Wenger JP, Omburo SN, Soto-Fuentes W, He J, Gang DR, Weiblen GD, Dixon RA (2009). "Identification of candidate genes affecting Δ9-tetrahydrocannabinol biosynthesis in Cannabis sativa". Journal of Experimental Botany. 60 (13): 3715–26. doi:10.1093/jxb/erp210. PMC 2736886. PMID 19581347.
- ↑ Baker PB, Taylor BJ, Gough TA (June 1981). "The tetrahydrocannabinol and tetrahydrocannabinolic acid content of cannabis products". J Pharm Pharmacol. 33 (6): 369–72. doi:10.1111/j.2042-7158.1981.tb13806.x. PMID 6115009.
- ↑ Schwilke EW, Schwope DM, Karschner EL, Lowe RH, Darwin WD, Kelly DL, Goodwin RS, Gorelick DA, Huestis MA (2009). "Δ9-Tetrahydrocannabinol (THC), 11-Hydroxy-THC, and 11-Nor-9-carboxy-THC Plasma Pharmacokinetics during and after Continuous High-Dose Oral THC". Clinical Chemistry. 55 (12): 2180–2189. doi:10.1373/clinchem.2008.122119. PMC 3196989. PMID 19833841.
- ↑ Röhrich J, Schimmel I, Zörntlein S, Becker J, Drobnik S, Kaufmann T, Kuntz V, Urban R (2010). "Concentrations of Δ9-Tetrahydrocannabinol and 11-Nor-9-Carboxytetrahydrocannabinol in Blood and Urine After Passive Exposure to Cannabis Smoke in a Coffee Shop". Journal of Analytical Toxicology. 34 (4): 196–203. doi:10.1093/jat/34.4.196. PMID 20465865.
- ↑ Baselt, R. (2011). Disposition of Toxic Drugs and Chemicals in Man (9th ed.). Seal Beach, CA: Biomedical Publications. pp. 1644–8.
- ↑ "Interview with the winner of the first ECNP Lifetime Achievement Award: Raphael Mechoulam, Israel". February 2007.
- ↑ Geller, Tom (2007). "Cannabinoids: A Secret History". Chemical Heritage Newsmagazine. 25 (2). Archived from the original on 19 June 2008.
- ↑ 51 Fed. Reg. 17476 (1986), Tuesday, May 13, 1986, pages 17476-17478
- ↑ Calhoun SR, Galloway GP, Smith DE (1998). "Abuse potential of dronabinol (Marinol)". Journal of Psychoactive Drugs. 30 (2): 187–96. doi:10.1080/02791072.1998.10399689. PMID 9692381.
- ↑ "Petition to Reschedule Cannabis (Marijuana)" (PDF). Coalition for Rescheduling Cannabis. 9 October 2002.
- ↑ "WHO Expert Committee on Drug Dependence". World Health Organization. Retrieved 12 January 2014.
- ↑ EMCDDA, ELDD Comparative Study, May 2002.
- ↑ "Marinol – the Legal Medical Use for the Marijuana Plant". Drug Enforcement Administration. Archived from the original on 21 October 2002. Retrieved 20 April 2011.
- ↑ Alchimia Blog, Marijuana and Medicine: Cesamet, Marinol, Sativex
- ↑ Downs, David (21 October 2014). "War on marijuana unconstitutional, doctors testify in federal court Monday". sfgate.com. Retrieved 21 October 2014.
- ↑ Eustice, Carol (12 August 1997). "Medicinal Marijuana: A Continuing Controversy". About.com. Retrieved 20 April 2011.
- ↑ Aizpurua-Olaizola, Oier; Soydaner, Umut; Öztürk, Ekin; Schibano, Daniele; Simsir, Yilmaz; Navarro, Patricia; Etxebarria, Nestor; Usobiaga, Aresatz (2016-02-26). "Evolution of the Cannabinoid and Terpene Content during the Growth of Cannabis sativa Plants from Different Chemotypes". Journal of Natural Products. 79 (2): 324–331. doi:10.1021/acs.jnatprod.5b00949. ISSN 0163-3864.
- ↑ Pickens JT (1981). "Sedative activity of cannabis in relation to its delta'-trans-tetrahydrocannabinol and cannabidiol content". British Journal of Pharmacology. 72 (4): 649–56. doi:10.1111/j.1476-5381.1981.tb09145.x. PMC 2071638. PMID 6269680.
- ↑ Burns TL, Ineck JR (2006). "Cannabinoid Analgesia as a Potential New Therapeutic Option in the Treatment of Chronic Pain". Annals of Pharmacotherapy. 40 (2): 251–260. doi:10.1345/aph.1G217. PMID 16449552.
- ↑ MARINOL (dronabinol) capsule drug label/data at Daily Med from U.S. National Library of Medicine, National Institutes of Health.
- ↑ McKim, William A (2002). Drugs and Behavior: An Introduction to Behavioral Pharmacology (5th ed.). Prentice Hall. p. 400. ISBN 0-13-048118-1.
- ↑ Greenberg, Gary (1 November 2005). "Respectable Reefer". Mother Jones. Retrieved 8 April 2010.
- ↑ "Cannabis and Cannabinoids (PDQ®)". Cancer Topics. National Cancer Institute, U.S. Department of Health and Human Services.
- ↑ "Government eases restrictions on pot derivative". Online Athens. Retrieved 12 January 2014.
- ↑ "Medical Marijuana". Multidisciplinary Association for Psychoactive Substances. Retrieved 12 January 2014.
- ↑ Gesellschaft für klinische Forschung e. V. (GKF) Unsere Projekte: Forschungsprojekte mit Cannabis-Extrakt Page accessed March 26, 2016
- ↑ Brownjohn PW and Ashton JC. Cannabinoids and Neuropathic Pain. Chapter 4 in Neuropathic Pain, ed Chukwunonye Udeagha, Cyprian. InTech, 2012. ISBN 978-953-51-0452-0
- ↑ Zajicek JP et al, with the MUSEC Research Group. Multiple sclerosis and extract of cannabis: results of the MUSEC trial. J Neurol Neurosurg Psychiatry. 2012 Nov;83(11):1125-32. PMID 22791906 Free full text
- ↑ Krishnan S, Cairns R, Howard R (2009). Krishnan S, ed. "Cochrane Database of Systematic Reviews". Cochrane database of systematic reviews (Online). Chapter = Cannabinoids for the treatment of dementia (2): CD007204. doi:10.1002/14651858.CD007204.pub2. PMID 19370677.
External links
| General | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Usage |
| ||||||||||||||||||
| Preparations | |||||||||||||||||||
| Extracts by potency | |||||||||||||||||||
| Consumption | |||||||||||||||||||
| Phytocannabinoids | |||||||||||||||||||
| Effects | |||||||||||||||||||
| Culture |
| ||||||||||||||||||
| Pro-Cannabis organizations | |||||||||||||||||||
| Use demographics | |||||||||||||||||||
| Politics |
| ||||||||||||||||||
| |||||||||||||||||||